This web page was produced as an assignment for Genetics 677, an undergraduate course at UW-Madison.
Heterozygous germline mutations in BMPR2, encoding a TGF- beta receptor, cause familial primary pulmonary hypertension
Written by The International PPH Consortium, Kirk B. Lane, Rajiv D. Machado, Michael W. Pauciulo, Jennifer R. Thomson, John A. Phillips III, James E. Loyd, William C. Nichols, and Richard C. Trembath
Reviewed by Ah Ram Kim
Reviewed by Ah Ram Kim
| scientific_journal.pdf |
The article “Heterozygous germline mutations in BMPR2, encoding a TGF- β receptor, cause familial primary pulmonary hypertension” is written by the International PPH Consortium, Kirk B. Lane, Rajiv D. Machado, Michael W. Pauciulo, Jennifer R. Thomson, John A. Phillips III, James E. Loyd, William C. Nichols, and Richard C. Trembath. This scientific journal emphasizes background of the research and the disease, methods, results, and their implications.
The condition of primary pulmonary hypertension (PPH) is defined as higher blood pressure than normal mean (> 25 mmHg at rest and > 30 mmHg during exercise). One of causes of familiar primary pulmonary hypertension (FPPH) is mutation on BMPR2, which is inherited in autosomal dominant manner. According to their research, proliferation of endothelial and smooth muscle cells causes blood pressure to elevate than normal pressure. This phenomenon of proliferation of cells is due to the mutation on the gene BMPR2. In order to identify the associated gene of PPH, they mapped on chromosome 2, locus of 2q33. This region was determined based on previous study. Using DNA from 8 PPH patients with family medical history by BAC/PAC mapping, 5.8Mb in PPH region at locus 2q33 was sequenced to identify candidate associated genes. A few candidate genes in the region were sequenced, such as Casp10, CTLA4, CD28, PSMA2, and BMPR2. After their intense analysis, they found that BMPR2 is the only gene that is associated with FPPH. BMPR2 encodes TFG- β type II family receptors. In normal state, TFG- β proteins bind to those receptors to activate serine/threonine kinase, which is an important during cell signaling. However, mutation on BMPR2 causes to fail to achieve a few events in cell signaling, such as failure ligand binding, blocking kinase activity, and destruction of heteromeric dimer formation. Briefly speaking, mutation on ENG and ACVRL1 at the gene BMPR2 destructs to encode TFG- β receptor that hinders cell signaling.
According to their genomic sequencing, a few different types of mutations were found. For example, they found 2 frameshift, 2 nonsense, and 3 missense mutations were found. More specifically, T residues in ATT repeating sequence in exon 12 was altered for frameshift mutation. In addition, the article emphasizes the consequences of those mutations. Due to these mutations, it hinders formation of heteromeric receptor complex between BMPR2 and BMPR1 at the cell surface via various mechanisms, such as disturbing ligand binding. Their further investigation shows missense mutations happen within the kinase domain. However, the question of how the missense mutation causes type II receptor to function properly is remained unanswered. Based on current research, they concluded that amino substation in kinase domain region effects negatively on its functionality.
The condition of primary pulmonary hypertension (PPH) is defined as higher blood pressure than normal mean (> 25 mmHg at rest and > 30 mmHg during exercise). One of causes of familiar primary pulmonary hypertension (FPPH) is mutation on BMPR2, which is inherited in autosomal dominant manner. According to their research, proliferation of endothelial and smooth muscle cells causes blood pressure to elevate than normal pressure. This phenomenon of proliferation of cells is due to the mutation on the gene BMPR2. In order to identify the associated gene of PPH, they mapped on chromosome 2, locus of 2q33. This region was determined based on previous study. Using DNA from 8 PPH patients with family medical history by BAC/PAC mapping, 5.8Mb in PPH region at locus 2q33 was sequenced to identify candidate associated genes. A few candidate genes in the region were sequenced, such as Casp10, CTLA4, CD28, PSMA2, and BMPR2. After their intense analysis, they found that BMPR2 is the only gene that is associated with FPPH. BMPR2 encodes TFG- β type II family receptors. In normal state, TFG- β proteins bind to those receptors to activate serine/threonine kinase, which is an important during cell signaling. However, mutation on BMPR2 causes to fail to achieve a few events in cell signaling, such as failure ligand binding, blocking kinase activity, and destruction of heteromeric dimer formation. Briefly speaking, mutation on ENG and ACVRL1 at the gene BMPR2 destructs to encode TFG- β receptor that hinders cell signaling.
According to their genomic sequencing, a few different types of mutations were found. For example, they found 2 frameshift, 2 nonsense, and 3 missense mutations were found. More specifically, T residues in ATT repeating sequence in exon 12 was altered for frameshift mutation. In addition, the article emphasizes the consequences of those mutations. Due to these mutations, it hinders formation of heteromeric receptor complex between BMPR2 and BMPR1 at the cell surface via various mechanisms, such as disturbing ligand binding. Their further investigation shows missense mutations happen within the kinase domain. However, the question of how the missense mutation causes type II receptor to function properly is remained unanswered. Based on current research, they concluded that amino substation in kinase domain region effects negatively on its functionality.
Figure 1
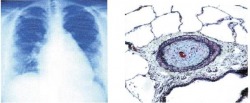
The left radiograph shows the increase of the right side of lung due to increasing workload in right ventricles and arteries. The right figure represents a lung biopsy of a PPH patient. Due to proliferation of endothelial and smooth muscle cells, the increased intima thickness reduces the size of vessel that blood should go through.
Figure 2 (retrieved from Figure 3 of the paper)
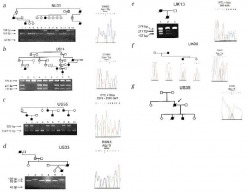
This figure shows how they analyzed different type of mutation—such as frameshift, nonsense, and missense mutation—in each patient.
Figure 3 (retrieved from Figure 4 of the paper)

This figure represents a different type of mutation in genomic sequence. Filled square-nonsense; filled circle-missense; filled triangle-frameshift. Asterisk-cysteine residue within the extracellular domain. Shaded region-encoding receptor kinase domain.
Scientific journal is written about their research and study and is addressing to scientists and expertise in this field. Therefore, their descriptions are detail and specific. In my opinion, I liked how they organized they research work in a paper. They stated what they found, what they are currently doing, and studies that need to carry on in future. They concluded their paper by stating connection between their research and clinical aspects. Providing numerical value helped authors to understand. For example, the definition of blood pressure is mentioned with providing the mean value of blood pressure. In addition, figures definitely helped readers understanding how genomic experiments were done and their significant results. As the purpose of providing figure, they sum up results in concise ways.
However, there are a few things they could improve in this paper. I personally think it would be better to state more details about their candidate genes. For instance, explaining how they are selected to be candidate genes that are associated with FPPH. Also, they should explain briefly why those genes are rejected by providing statistical value or any other experimental data. By explaining no association between other candidate gene and FPPH will support strongly the idea that the gene BMPR2 is the only one gene associating with FPPH.
However, there are a few things they could improve in this paper. I personally think it would be better to state more details about their candidate genes. For instance, explaining how they are selected to be candidate genes that are associated with FPPH. Also, they should explain briefly why those genes are rejected by providing statistical value or any other experimental data. By explaining no association between other candidate gene and FPPH will support strongly the idea that the gene BMPR2 is the only one gene associating with FPPH.
[1] The International PPH consortium, Lane, K. B., Machado, R., Pauciulo, M.W., Thomson, J.R., Phillips III, J.A., Loyd, J.E., Nichols, W.C., Trembath, R.C. (2000). Heterozygous germline mutations in BMPR2, encoding a TGF- β receptors, cause familial primary pulmonary hypertension. Nature genetics, vol 26, p.81-84.
doi:10.1038/79226
doi:10.1038/79226
